HIV Prevention in South Africa Enters New Era: Lenacapavir Rollout Begins as Cabotegravir Injection Phases Out
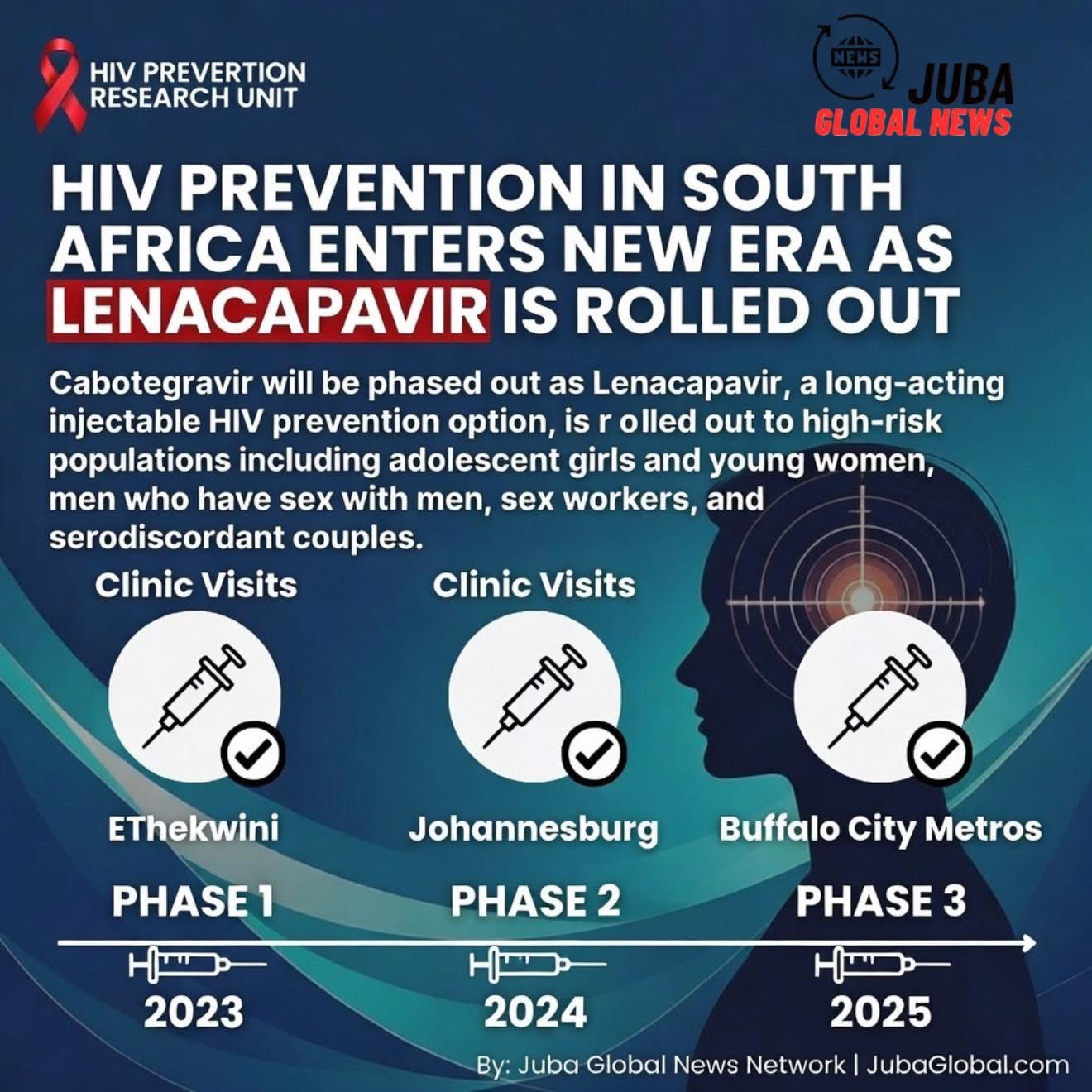
In March 2026, South Africa—the country with the world’s largest HIV epidemic—officially began the phased national rollout of lenacapavir (LEN), a long-acting injectable HIV pre-exposure prophylaxis (PrEP) drug developed by Gilead Sciences. The move marks a major shift in the country’s HIV prevention strategy, as the previously introduced long-acting cabotegravir (CAB-LA) injection is now being systematically phased out in public-sector programs.
With an estimated 7.8 million people living with HIV and roughly 150,000–170,000 new infections annually, South Africa has long been at the forefront of both treatment and prevention innovation. The transition to lenacapavir is seen as a potential game-changer for PrEP uptake, adherence, and impact among high-risk populations.
Background: The HIV Burden and Early PrEP Efforts
South Africa accounts for approximately 20% of the global HIV burden despite representing less than 1% of the world’s population. Key populations—adolescent girls and young women (15–24 years), men who have sex with men, sex workers, people who inject drugs, and serodiscordant couples—continue to drive new infections.
Daily oral PrEP (tenofovir/emtricitabine) was introduced in the public sector in 2016 and scaled up significantly after 2020. By 2025, over 1.2 million people had initiated oral PrEP at least once, but real-world adherence remained a major challenge: many users discontinued within months due to pill fatigue, stigma, forgetfulness, or side effects.
In 2023–2024, South Africa became one of the first African countries to introduce long-acting cabotegravir (CAB-LA), marketed as Apretude, administered every two months. CAB-LA demonstrated superior efficacy over oral PrEP in clinical trials (HPTN 083 and 084), reducing HIV incidence by more than 60–70% compared with daily pills. However, rollout faced significant hurdles:
- High cost (initially >$200 per dose in low- and middle-income settings)
- Cold-chain requirements
- Limited supply
- Injection-site reactions
- Logistical complexity in rural clinics
By late 2025, only a few hundred thousand doses had been administered in the public sector, far short of targets.
Enter Lenacapavir: Twice-Yearly Protection
Lenacapavir, approved by the U.S. FDA in 2022 for treatment and granted tentative approval for PrEP in 2024, offers a twice-yearly subcutaneous injection (every six months). The PURPOSE 1 and PURPOSE 2 trials (conducted in South Africa, Uganda, and other sites) showed near-perfect efficacy: zero infections among women and men receiving LEN in the blinded phase, compared with multiple infections in oral PrEP arms.
Key advantages of lenacapavir over cabotegravir include:
- Twice-yearly dosing (vs. every two months) → dramatically lower clinic visit burden
- No cold-chain requirement (stable at room temperature)
- Lower projected cost once generic versions are scaled (Gilead has signed voluntary licensing agreements with six generic manufacturers for low- and middle-income countries)
- High acceptability in trial participants, particularly among young women
In late 2025, the South African Health Products Regulatory Authority (SAHPRA) granted full approval for lenacapavir for PrEP. The National Department of Health (NDoH) subsequently announced that LEN would become the preferred long-acting PrEP option in the public sector starting in Q1 2026.
The Phase-Out of Cabotegravir
Cabotegravir (CAB-LA) is not being withdrawn from the market entirely, but its public-sector rollout is being deprioritized and gradually phased out:
- Existing CAB-LA users will be offered transition to LEN at their next scheduled visit.
- New initiations of CAB-LA in public clinics have largely stopped since February 2026.
- Remaining CAB-LA stock is being used to complete courses for those already on it.
- Private-sector access to CAB-LA continues for those who can afford it or prefer it.
The decision was driven primarily by logistics and cost-effectiveness: LEN requires only two clinic visits per year compared with six for CAB-LA, significantly reducing transport, staffing, and supply-chain costs in under-resourced facilities.
Rollout Plan and Early Implementation
The NDoH’s 2026–2027 PrEP Implementation Plan prioritizes:
- Adolescent girls and young women (15–24) in high-incidence districts (KwaZulu-Natal, Gauteng, Eastern Cape, Mpumalanga)
- Key populations in urban hotspots (men who have sex with men, sex workers, transgender people)
- Serodiscordant couples and pregnant/breastfeeding women
Initial rollout sites include:
- High-volume primary health clinics in eThekwini, Johannesburg, and Buffalo City metros
- Mobile outreach teams in rural KwaZulu-Natal and Eastern Cape
- University and TVET college health services
- Sex-worker programs in Gauteng and Western Cape
Training for nurses and community health workers began in January 2026, focusing on injection technique, eligibility screening, adherence counseling, and management of rare side effects.
Early data from pilot sites in KwaZulu-Natal (February–March 2026) show:
- High acceptance: >85% of eligible women offered LEN agreed to start
- High retention: >90% returned for the second injection at six months
- Very low discontinuation due to side effects (<3%)
Challenges and Remaining Barriers
Despite the excitement, several obstacles remain:
- Supply constraints: Initial volumes are limited; full national scale-up will take 12–24 months.
- Injection-site reactions: Mild to moderate pain, swelling, or nodules occur in ~10–15% of recipients (usually resolve within days).
- Stigma: Fear of being seen attending clinics for “HIV drugs” persists among young people.
- Integration with other services: Linking PrEP to contraception, STI screening, and gender-based violence support is critical but uneven.
- Cost sustainability: Even with generic production, long-acting injectables remain more expensive than oral PrEP; donor transition plans must be carefully managed.
Looking Ahead
If South Africa can successfully scale lenacapavir, it could become the first large-scale, real-world demonstration of twice-yearly HIV prevention at population level. Modeling studies estimate that achieving 30–40% coverage among young women in high-incidence areas could avert tens of thousands of new infections annually.
The transition from cabotegravir to lenacapavir is not just a change in drug—it is a strategic pivot toward longer-acting, lower-frequency prevention tools that better match the realities of people’s lives.
For millions of South Africans still at risk, 2026 may mark the beginning of a new chapter in the fight against HIV—one where protection arrives just twice a year, rather than every day.
By Juba Global News Network | JubaGlobal.com
March 16, 2026